
A comparative study of the functional fitness and perception of quality of life among elderly participants and non-participants of Universities of third age
Un estudio comparativo de la condición física funcional y de la percepción de cualidad de vida entre los ancianos frecuentadores y no-frecuentadores de Universidad de la tercera edad
Authors
Biehl-Printes, Clarissa 1; Teixeira, Diogo 1; Costa, Armando 1; Pinheiro, Valter1; Sousa, Paulo 1; Cruz, Joana2; Tomas-Carus, Pablo 3
1 Departamento de Ciências do Desporto. Instituto Superior de Ciências Educativas – ISCE. Lisboa. Portugal
2 Departamento Social e Cultural. Instituto Superior de Ciências Educativas – ISCE. Lisboa. Portugal
3 Departamento de Ciências do Desporto e Saúde, Universidade de Évora. Évora. Portugal
Corresponding Author:
Clarissa Biehl Printes, cbprintes.isce@gmail.com
Departamento de Ciências do Desporto.
Instituto Superior de Ciências Educativas – ISCE.
Odivelas, Lisboa
Author contributions
Biehl-Printes C. conceived of the study, participated in its design and coordination, analysed the data, contributed to the results discussion and wrote the manuscript; Teixeira D., analysed the data and contributed to the results discussion; Costa A., Pinheiro V., and Sousa P., contributed to the results discussion; Cruz J., participated in coordination and data collection. Tomas-Carus P., participated in the study design and coordination, and contributed to the results discussion. All authors read and approved the final manuscript.
Abstract
Objectives: To analyze the contributions of Universities of third age (U3A) through their proposed activities and effects in functional fitness and quality of life of elderly participants and non-participants.
Methods: The sample was composed of two groups: elderly participants in U3A (EPG; n=25) and elderly non-participants (ENPG; n=25). Data collection was obtained through questionnaires: one about sociodemografic characteristics and U3A attendance (General questionnaire) and another about quality of life (WHOQOL-BREF Portuguese version). Also, were applied two test of the Fullerton Tests battery (30-second chair stand and 8-food up and go).
Results: The results show statistically significant differences in attendance between women (76%) and men (24%). There is a predominance of married (68%) that attend the U3A. The educational level indicates that the EPG present more years of education (28%) and more people with higher education (24%). The main reason why the ENPG didn’t attend U3A was lack of time (44%). For lower body strength, the results showed differences between EPG and ENPG (p=0.022), in favor of EPG. No differences were observed between groups for agility/dynamic balance (p=0.977). In quality of life were observed differences between groups in the physical domain (p=0.026), with the EPG presenting higher scores that ENPG. For all the other domains, no differences were observed (all p>0.050).
Conclusions: This study showed a prevalence of attendance of women to U3A and that the enrolled elderlies have more previous years of schooling. The elderly participants in U3A showed better physical domain than non-participants. However, in other domains were not found differences between participants and non-participants. For future studies, it is proposed that the sample should encompass groups with higher age range that may produce results with new interpretations.
Keywords: active aging; university of third age, functional fitness, quality of life.
Resumo
Objetivos: Analisar as contribuições da Universidade da Terceira Idade (UTI) através de suas atividades propostas e os efeitos na aptidão funcional e qualidade de vida dos idosos participantes e não-participantes.
Métodos: A amostra foi composta por dois grupos: idosos participantes na UTI (GIP; n=25) e idosos não-participantes (GINP). A coleta de dados foi obtida por meio de questionários: um sobre as características sóciodemográficas e particpação na U3A (questionário geral) e outro sobre a qualidade de vida (WHOQOL-BREF versão Portuguesa). Além disso, foram aplicados dois testes da bateria Fullerton Tests (30-chair stand and 8-food up and go).
Resultados: Os resultados mostraram diferenças estatísticas significativas na participação entre as mulheres (76%) e homens (24%). Há um predomínio de casados (68%) dos idosos que participam na U3A. O nível de escolaridade indica que os idosos do GIP apresentam mais anos de escolaridade (28%), e mais idosos com ensino superior (24%). A principal razão pela qual o GINP não adere a U3A está associada à falta de tempo (44%). Para aptidão física funcional, os resultados mostraram diferenças entre o GIP e GINP (p=0.022) para uma menor força do corpo. Não foram observadas diferenças entre os grupos para a agilidade/equilíbrio dinámico (p=0.977). Na qualidade de vida foram obeservadas diferenças entre os grupos no domínio físico (p=0.026), valores mais elevados no GIP. Para todos os outros domínios não foram encontradas diferenças (todos p>0,050).
Conclusões: Este estudo mostrou uma prevalência de participação das mulheres na U3A, e que os idosos inscritos têm mais anos e nível de escolaridade. Os idosos participantes mostraram melhor domínio físico que os não-participantes. No entanto nos outros domínios não foram encontradas diferenças. Para estudos futuros, propõe-se uma amostra com uma faixa etária mais elevada, de modo a possibilitar outro tipo de resultados sujeitos a novas interpretações.
Palavras chaves: envelhecimento ativo, universidade sénior, aptidão física funcional, qualidade de vida.
Introduction
World population age has arisen in the last decades. Despite this, several conquests were made in modern societies as a mean to adjust to this new social paradigm. It is possible to observe that these populations are experiencing the challenge of an active aging. It is commonly accepted that a person with 65 or more years old is considered an elderly individual (3rd age), but new definitions arise in order to adjust to the prolonged life expectancy and to better distinguish among the vast amplitude previously existing. For this matter, a new stratification now seems to be consensual, ranging between 80-85 or more years (i.e. 4th age) ( Formosa, 2012; Stathi & Simey, 2007).
In Europe changes in this age group has been a matter of concern and interest for more than 40 years, in which France stood as one of the countries to boost successful aging trough higher education institutions (Cachioni, 2012; Lemieux, Boutin, Snachez & Riendeau, 2003). In the 70’s Portugal, alongside France, implemented the concept and practice of free time associations denominated Universities of 3rd Age (U3A) or Senior Universities (SU), but adopted an English structured model based in non-profit associations or self-organized groups, with non-formal education, differing from the French model associated with formal Universities (Jacob, Jesus & Sampaio, 2012; Lemieux et al., 2003; Pinto, 2003).
Gradually, the chronologic concept adopted by U3A and SU in the 60’ and 70’ decades that referred this association as a socio-educative response to individuals starting 50 years of age, has been weakened by the senescence age attributed in the 80’ decade by OMS of 60 and 65 years (Jacob et al., 2012; OMS, 1980; ONU, 1982). However, that socio-educative response, targeting the creation and dynamization of regular social, cultural, educational, physical and socializing activities reflect a perfect integration of the previously framework if the active aging concept previously proposed by OMS (1990), that envisions as a major objective to create opportunities to optimize conditions to health, participation and security, that may allow the quality of life as people become older (Jacob et al., 2012; WHO, 2002).
Data from Portuguese senses tends to show a crescent trend in the number of people with more than 65 years (19.1% of the population), surpassing that of young (15%), accentuating the verified trend in 2001 senses (Carrilho & Patrício, 2010). Due to the evidence that elderly people are increasing, it becomes even more relevant to stimulate programs and politics of healthy aging, assuring the continuities of a productive, healthy and quality life. Therefore, the concept of quality of life in the advanced age is considered as one of main indicators to evaluate the condition of life of the elderly, involving different dimensions that encompass the optimum level of physical, mental, social, performance functioning, and satisfaction with life and their well-being (Fleck et al., 2000; Fonseca, 2005). Corroborating the perspective of a comprehensive concept of quality of life that involve a wide array of multidisciplinary perspectives (e.g. sociologic, biomedical, psychological, economical and environmental) (Walker, 2005), interested investigate the contribution that the social support networks that allow organization of 3rd age activities (i.e. U3A/SU) brings to functional health, independent life, social relations and to psychological well-being of these people. As an example, previous studies show that adherence to these organizations influence physical and psychological well being. In this sense, an association between the participation in U3A and a lower intensity depression was found (Irigaray & Schneider, 2007). The interest in physical activities practices and the pursuance of well-being was demonstrated as a determinant indicator of the U3A participants, as for a better perception of the factors related to the environmental and psychological domains and global perception of quality of life and health in middle age and elderly people (Castro et al., 2007; Fenalti & Swartz, 2000).
To the extent of our knowledge, it seems to exist a discrepancy between the high number of U3A/SU in Portugal (over 200 registered in 2012) and scientific work published within this approach (5). Several studies are unanimous to assume the influence of an active life style with some variability of physical and cognitive activities to the promotion of the quality of the lived years (Colombe & Krower, 2003; Chou, Hwang & Wu, 2012). In these sense, the multidisciplinary set offered by U3A in physical activities, such as physical education, walking, dancing, yoga and senior bocce are normally available to elderly students.
Thus, assuming U3A as a prepared organization with a wide array of multidisciplinary opportunities with continuous and regular formation, we ought to explore these contexts and develop scientific knowledge to ensure the promotion and valorization required to continue a healthy and active aging. Therefore, in this study we propose to analyze the contributions of U3A through their proposed activities and effects in physical fitness and quality of life elderly people.
Material and Methods
Sample selection
For this exploratory cross-sectional study were used posters and verbal communication to call for voluntary participants in Senior University of Odivelas (SUO), integrated in Superior Institute of Educational Sciences (ISCE). Selection criteria were: men and women >65 years, elderly participants of SUO (EPG; n=25) and elderly non- participants (ENPG; n=25 – elderly friends and family of the participants of SUO – we asked participants of U3A to bring to the evaluation day a friend or family member) without cognitive and locomotors problems (we allowed the participation of elderlies that used a canadian cane). Exclusion criteria: elderly that already attending another U3A or other social organization for 3rd age (i.e. sports club, social solidarity association, inhabitant association) or those that participate in entities or organizations directed to this population (i.e. day centers, recreational collectivities, municipal services). The participants were informed of study procedures and given the informed consent to voluntary participate in the research. All were approved by the Ethics Committee of Health and Welfare of the University of Évora (Document Nº 13020) and were in accordance with the 1975 Helsinki Declaration.
Procedures and instruments
Sociodemographic characteristics, cognitive problems and adherence to the U3A
All participants were asked about the age, civil status and education level. Immediately, the Watch Design Test (Freitas & Simões, 2010) was used as exclusion criteria for cognitive problems in the elderly. Each participant was asked to make a clock (no pre-defined time), making a circle and putting the numbers in the correct position, without looking in to his watch. When finished, it is asked to put the indicators marking 10 minutes to 2 o’clock. This test is used to evaluate: visual perception, construction praxis, right hemisphere dysfunction and left hemisphere negligence. For example: small watch indicates lack of planning and inadequate positioned numbers point to executive deficit. Additionally, was analyzed the characteristics of adherence to the U3A by the senior participants. Only the EPG were asked about years attends U3A, times per week, motivational factors, intent of leaving and number of disciplines attended. The ENPG were asked about the reasons why they didn’t attend U3A.
Quality of Life
The Portuguese version of World Health Organization Quality of Life Group (WHOQOL-Bref) (Fleck et al., 2000) was applied to assess quality of life. This instrument has 26 questions divided in four domains of quality of life: physical capacity, psychological well-being, social relations and the environment where the individual is inserted. Besides these four domains, WHOQOL-Bref it is also composed by a domain that assesses global quality of life. Each domain is composed by questions where higher scores (between 1 and 5) represent better quality of life. Some characteristics, designed as facets are not formulated in a positive sense. In these cases higher scores do not mean better quality of life. Scoring is calculated by a syntax that considers answers in each question composing the domain, resulting in final scores in a scale of 4 to 20, comparable to dose of WHOQOL-100, which can be transformed in a 0 to 100 scale.
Functional fitness
For assess lower body strength and agility/dynamic balance were applied two test of Fullerton Functional Fitness Test Battery (Rikli & Jones, 1999): 30-Second Chair Stand and 8-Foot Up and Go. The 30-Second Chair Stand Test assess lower body strength, needed for numerous tasks such as climbing stairs, walking and getting out of a chair, tub or car. The elderly people should perform the maximum number of full stands that can be completed in 30 seconds with arms folded across chest. The 8-Foot Up and Go Test assess agility/dynamic balance, which is important in tasks that require quick manoeuvring, such as getting off a bus in time or getting up to attend to something in the kitchen, to go to the bathroom or to answer the phone. The elderly people should to get up from a seated position, walk 2.44 metres (8 foot) and return to seated position.
Statistical analysis
Normality of data was initially tested using the Kolmogorov-Smirnov test. Differences between groups were tested using Kruskal-Wallis test for continuous variables (age, functional fitness and quality of life) and Chi-square test for categorical variables (sex, civil status, educational level). For all tests the significance level was set at p<0.05. These analyses were performed in SPSS 22.0 software.
Results
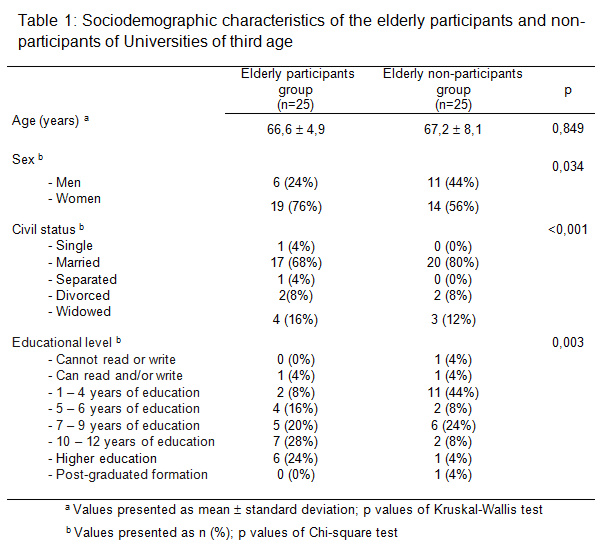
Sociodemographic characteristics
Were observed significant differences between EPG and ENPG in sex, civil status and educational level. The results showed that the women’s attend more U3A than men. Also was showed that there is a predominance of married elderly that attend the institution. The educational level indicates that the elderly in the EPG present more years of education and more people with higher education (Table 1).
Additionally, we have analyzed the characteristics of adherence to the U3A by the EPG. We observed that our sample attends U3A for 3,88 ± 1,76 years with a frequency of 3,48 ± 1,12 times per week; the three more motivational factors were 1) own will – 18 (72%), 2) refer of a friend – 4 (16%) and 3) refer of family – 2 (8%); the intent of leaving U3A 1) Yes – 1 (4%) and No – 24 (96%); number of disciplines attended was 4,44 ± 1,63; the five more attended disciplines were 1) Music – 13 (52%), 2) English – 12 (48%), 3) Painting – 11 (44%), 4) Informatics – 10 (40%) and 5) Spanish – 8 (32%). We also asked the ENPG the reasons why they didn’t attend U3A, being that the three main reasons were 1) lack of time – 11 (44%), 2) does not consider an adequate ambient for themselves – 8 (32%),3) financial limitations – 3 (12%) and 4) locomotors difficulties – 1 (4%).
Functional fitness and Quality of life
Were showed significant differences between EPG and ENPG in lower body strength. The EPG showed more strength in the lower body. No differences were observed between groups in agility/dynamic balance. In addition, were observed differences between groups in the physical domain (p=0.026), with the EPG presenting higher scores that the ENPG. For all the other domains, no differences were observed between groups. Nonetheless, the EPG presents marginally higher scores in three other of the five non-statistically significant variables (perception of overall quality of life, psychological domain and social relationships domain) (Table 2).
Discussion
This comparative study showed that the more women go to U3A and that elderly enrolled have more previous years of schooling. The frequency engage in activities was of 3 times/week and there is no report of intention the leave the U3A after enrolling. Non-enrolled elders consider the lack of time the main cause preventing them to start in U3A. The participants in U3A showed better strength and quality of life in physical domain that non-participants in U3A. However, in all domains they present a “good” classification in quality of life.
The data presented in the sociodemographic analysis supports previous findings. The age, sex and level of education distribution in our EPG is in accordance with studies done in other countries that have functioning U3As and have demographic similarities with Portugal (Alfageme, 2007; Formosa, 2012; Mindwinter, 1996). In our study, the mean age is clearly within the 3rd age group for elderly men and women, women are the highest percentage of members in U3A and the participants have higher levels of education. This is an expected trend repeatedly presented in previous studies. This generally represents the retirement age of this population, the absence of similar services in this age group, higher life expectancies for women, and a set of secondary and post-secondary education experiences that may have influenced the motivations and pleasure associated with learning in the past, contrasting with the heavy class baggage associated with the name “university” for the owners of lower education levels (Formosa, 2012).
The U3A provides a space that has multidimensional and multidisciplinary interactions with the elderly people. The range of disciplines provided promotes an interaction that allows the training and development of physical, social, cultural and psychological domains. The combination of disciplines attended by the elderly will ultimately define the benefits obtained (Pinto, 2003). As seen in ours results, the participants in U3A tend to enrolled in the institution by self-initiative, of the thirty disciplines they attend in average 4, were the most frequented are music, painting, informatics, English and Spanish, all promoters of sedentary or light physical activity during class time. However, these activities are promoters of a high cognitive and motor-cognitive function, marked today as important to this population. Several studies have indicated that cognitive training have advantages to retard the cognitive decline in the process of healthy aging, were new technologies like computers and video games present themselves as alternatives of intervention to be expanded (Kueide, Parisi, Gross, & Rebok, 2012). Additionally, it is suggested that cognitive domain practices may bring gains in the cognitive performance of healthy elderlies that may manifest 5 years after training (Willis et al., 2006). Moreover, previous studies support the efficacy of the practice of motor coordination activities, trough gross and fine motor abilities activation, that act positively in executive functions that may seem to be independent of gains obtain by cardiovascular and strength training (Voelcker-Rehage, Godde & Staudinger, 2011; Yan & Zhou, 2009). Physical activities are presented in several disciplines and by different modalities, where students presented their preference in boccia (20%), dance (20%) and physical activities (12%), which in general shows an adherence as significant as music, languages, painting and informatics. However, bearing in mind the several possible ways to promote a healthy and active aging, it is suggested and supported the pertinence of each filed of intervention, either by cognitive abilities, motor-cognitive associated with physical exercise, physical activities, social relation, nutrition, etc., all contributing to retard the cognitive decline associated to the loss of functional independence, autonomy and quality of life (Williams & Kemper, 2010).
The participants in U3A showed better quality of life in physical domain that non-participants. This domain explores pain and discomfort, energy and fatigue and stress and rest facets (Fleck et al., 2000). From the data collected it is not possible to clearly identify the reasons behind this result. One factor that may be influencing the higher results presented in physical domain by the EPG is the lower body strength score. It is possible to observe that there were differences between groups in this parameter, in favor of EPG. However, all domains quality of life showed a classification of “good” (score ≈75 in scale 0-100), this could be due to the age (years) of the attendees 66,6 (EPG) and 67,2 (ENPG), functional and mental conditions adequate to an independent and active life that may have a low interference in quality of life. This, associated with the concept that aging is a dynamic and progressive process that involve physical, functional, biochemical, psychological and social changes that, when associated with an active healthy life style, results in a bigger longevity, described in previous studies (Castro et al., 2007; Chodzko-Zajko & Schwingel, 2009; Ferreira, Maciel, Costa, Silva & Moreira, 2012). Several studies pointed out the importance of U3A in promoting health benefits for their members (Formosa, 2012; Ordonez, Lima-Silva & Cachioni, 2011; Sonati, Modeneze, Vilarta, Maciel & Boccalett, 2011), and that there is a positive relationship between psychological wellbeing and participating in U3A with extension to other areas of life (Maniecka-Bryłaemail, Gajewska, Burzyńska, & Bryla, 2013). Additionally, EPG shows a sustained connection to U3A with the duration of 4 years, assuming a frequency of 3 times per week, reflecting the capability for retaining for a long period elderlies in activities. Continuous adherence of elderly in health promoting activities is the question of interest in this research, considered as problematic for the shift in the healthy life style (Caetano & Raposo, 2005). For this matter, it seems interesting to point out that U3A is a promoter of this change.
The present study also included limitations, which require further discussion. First, the age in the group studied may have influenced the results, regarding that they already enjoy good functional, mental and physical health, associated with quality of life. Besides, ENPG considers that they do not attended U3A mainly because of lack of time (44%), maintaining themselves active and involved in other activities, being, this way, equally active to EPG, condition that influence directly in the evaluation of quality of life. Another possible analysis to be considered on sociodemographic variables is labor situation (i.e. working; retired). The association with work and health is well documented, where labor activities are seen as having a positive role in preservation some health variables, whereas unemployment is associated with higher rates of mortality, psychiatric symptoms and worst health conditions (Arber, 1987; Janlert, 1997). Few studies had addressed this theme with elderly. Findings described on the relation of the capacity of sustaining a healthy living associated with non-formal work, sociodemographic characteristics, higher levels of schooling, health condition, autonomy and independence (Giatti, & Barreto, 2003; Marmot & Shipley, 1986). However, and in U3A context, we consider this study as pioneer in elderly and quality of life characterization.
Conclusion
This study showed a higher adherence of women to U3A and that elderly enrolled have more previous years of schooling. Additionally, the participants in U3A engage in activities with a weekly frequency on average of 3 times and there is no report of intention the leave the U3A after enrolling. The ENPG considered the lack of time the main cause preventing them to start in U3A. Moreover, were observed higher levels in lower body strength and physical domain in participants of U3A. However, in all domains they present a good classification in quality of life. We propose the development of studies with higher age groups, mainly because they may possess different characteristics and present results worthy of new interpretations.
Acknowledgements
We would like to thank Direction of Senior University of Odivelas for allow us to develop this study, and to the elderly that collaborate voluntary in this study.
References
- Formosa, M. (2012). Four decades of Universities of the Third Age: past, present, future. Ageing and Society, 34(1), 42-66.
- Stathi, A & Simey, P. (2007). Quality of life in the Fourth Age: exercise experiences of nursing home residents. Journal of Aging and Physical Activity, 15 (3), 272-286.
- Lemieux, A. Boutin, G. Sanchez, M. & Riendeau, J. (2003). The faculties of education in the traditional universities and the third age universities: A model of partnership. Versão policopiada. 9: 2.
- Cachioni, M. (2012). Universidade da Terceira Idade: história e pesquisa. Revista Temática Kairós Gerontologia, 15 (7), 01-08.
- Jacob, L. Jesus, A. & Sampaio, J. (2012). Universidades Seniores: criar novos projetos de vida. Lisboa: Ed. Rutis.
- Pinto, M. (2003). As Universidades da Terceira Idade em Portugal: das origens aos novos desafios no futuro. Revista da Faculdade de Letras – Línguas e Literaturas, 20(2), 467-478.
- Organización Mundial de la Salud (1980). Informe de la conferencia preparatoria de la OMS para a asamblea mundial de las naciones unidas sobre el envejecimiento. México.
- Organização das Nações Unidas (1982). Asamblea mundial sobre el envejecimiento. Viena
- World Health Organization (2002). Active ageing: A policy framework. Geneva.
- Carrilho, M. J. & Patrício, L. (2010). The demographic Changes in Portugal. Lisboa: National Institute of Statistics.
- Fonseca, A. M. (2005). O envelhecimento bem sucedido. In Paúl & A. Fonseca (Eds.). Envelhecer em Portugal.(pp. 281-311).Lisboa: Climepsi Editores:
- Fleck, P. A., Louzada, S., Xavier, M., Chachamovich, E., Vieira, G., Santos, L. & Pinzon V. (2000). Aplicação da versão em português do instrumento abreviado de avaliação da qualidade de vida “WHOQOL-bref”. Revista Saúde Pública, 34 (2), 178-83.
- Walker, A. A. (2005). European perspective on quality of life in old age. European Journal of Ageing, (2), 2-12.
- Irigaray, T. Q. & Schneider, R. H. (2007). Prevalence of depression in elderly women attending the University of Third Age. Revista Psiquiatria Rio Sul, 29(1),19-27
- Fenalti, R. C. & Shwartz, G. M. (2000). Universidade Aberta à Terceira Idade e a perspectiva de ressignificação do Lazer. Revista Paulista de Educação Física, 17(2),131-41
- Castro, P. C., Tahara, N., Rebelatto, J. R., Driusso, P., Aveiro, M. C. & Oishi, J. (2007). Influência da universidade aberta da terceira Idade (UATI) e do programa de revitalização (Revt) sobre a qualidade de vida de adultos de meia-idade e idosos. Revista brasileira de Fisioterapia, 11(6), 461-7.
- Colombe, S. & Kramer, A. F. (2003). Fitness effects on the cognitive function of older adults: a meta-analytic study. Psychological Science, 14, 125-30.
- Chou, C. H., Hwang, C.L., & Wu, Y. T. (2012). Effect of exercise on physical function, daily living activities, and quality of life in the frail older adults: a meta-analysis. Archives of Physical Medicine and Rehabilitation, 93(2), 237-44.
- Freitas, S. & Simões, M, R. (2010). Teste do desenho do relógio: utilidade e validade como instrumento de rastreio cognitivo. Psicologia, Educação e Cultura, 14(2), 319-37.
- Rikli, R. & Jones, J. (1999) Development and validation of a functional fitness test for community-residing older adults. Journal of Aging and Physical Activity, 7,129-161.
- Alfageme, A. (2007). The clients and functions of Spanish university programmes for older people: a sociological analysis. Ageing & Society, 27(03), 343-361.
- Mindwinter, E. (1996). Thriving people: The growth and prospects of the U3A in UK. London: Third Age Trust.
- Pinto, M. G. (2003). The current status and future prospects of university programmes for seniors in Southern and mediterranean Europe: the case of Portugal. Revista da Faculdade de Letras “Línguas e Literaturas”, Série II, vol. 20 (1), 71-90.
- Kueider, A. M., Parisi, J.M., Gross, A. L. & Rebok, G. W. (2012). Computerized Cognitive Training with Older Adults: A Systematic Review. PLoS one, 7, e40588.
- Willis, S. L., Tennstedt, S.L., Marsiske, M., Ball, K., Elias, J., Koepke, K.M., et al. Long-term effects of cognitive training on everyday functional outcomes in older adults. Jama. 296: 2805–2814.
- Yan, J. H. & Zhou, C, L. (2009). Effects of motor practice on cognitive disorders in older adults. European Review of Aging and Physical Activity, 6(2), 67–74.
- Voelcker-Rehage. C., Godde, B. & Staudinger, U. M. (2011). Cardiovascular and coordination training differentially improve cognitive performance and neural processing in older adults. Frontiers in Human Neuroscience, 17(5), 26.
- Williams, K. & Kemper, S. Exploring interventions to reduce cognitive decline in aging. Journal of Psychosocial Nursing and Mental Health Services. 2010; 48(5): 42–51.
- Ferreira, O.G.L., Maciel, S.C., Costa, S. M. G., Silva, A.O. Moreira, M. A. S. P. (2012). Envelhecimento ativo e sua relação com a independência funcional. Texto Contexto Enferm, Florianópolis. Jul-Set; 21(3): 513-8.
- Chodzko-Zajko, W., & Schwingel, A. (2009). Transnational Strategies for the Promotion of Physical Activity and Active Aging: The World Health Organization Model of Consensus Building in International Public Health. Quest, 61(1): 25-38.
- Sonati, J., Modeneze, D. M., Vilarta, R., Maciel, E. S. & Boccaletto, E. M. (2011). Body weight as an indicator of fat-free mass in active elderly women. Maturitas, 68(4), 378-81.
- Ordonez, T., Lima-Silva, T. & Cachioni, M. (2011). Subjective and Psychological well-being of students of University of the third age. Benefits of continuing education for psychological adjustment in the elderly, Dementia e Neuropsychologia, 5(3), 216-225.
- Maniecka-Bryłaemail, I., Gajewska, O., Burzyńska, M. & Bryla, M. (2013). Factors associated with self-rated health (SRH) of a University of the Third Age (U3A) class participants. Archives of Gerontology and Geriatrics, 57(2), 156-161.
- Caetano, L. M. & Raposo, J. V. (2005). Atitudes dos Idosos face à Actividade Física. Cuadernos de Psicología del Deporte, Vol. 5, núms. 1 y 2.
- Arber, S. (1987). Social class, non-employment, and chronic illness: Continuing the inequalities in health debate. British Medical Journal, 294, 1069-1073.
- Janlert, U. (1997). Unemployment as a disease and disease of the unemployed. Scandinavian Journal of Work, Environment & Health, 23, 79-83.
- Giatti, L. & Barreto, S. M (2003). Health, work, and aging in Brazil. Cadernos de Saúde Pública, 19(3), 759-771.
- Marmot, M. G. & Shipley, M. J., (1996). Do socioeconomic differences in mortality persist after retirement? 25 years follow up of civil servants from the Whitehall study. British Medical Journal, 313, 1177-1180.